Myelodysplastic syndromes (MDS)
MDS are a diverse and heterogeneous group of disorders characterised by ineffective haematopoiesis, dysplasia in haematopoietic cells, cytopenias and increased risk of progression to acute myeloid leukaemia.5,6 Over 80% of patients with MDS experience anaemia.7 Mutations involving signalling molecules, epigenetic regulators, splicing factors and transcription regulators are present in most cases of MDS.5
Below are the four video clips of experts discussing the mechanisms involved in chronic anaemia associated with MDS and β-thalassaemia
Parallels in ineffective erythropoiesis: MDS and β‑thalassaemia biology
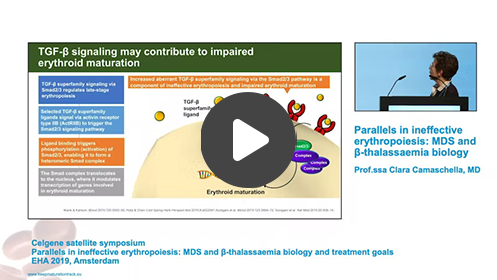
Professor Clara Camaschella, Professor of Internal Medicine and Haematology, Vita-Salute San Raffaele University
In this video, Professor Camaschella discusses some of the growth factors and transcription factors involved in erythropoiesis. Professor Camaschella describes the role of GATA‑1 and the transforming growth factor (TBF‑β) superfamily in the erythropoiesis process and in the ineffective erythropoiesis that plays a key part in the chronic anaemia observed in MDS and β-thalassaemia.
6-minute video
Burden of anaemia and chronic transfusions

Professor Maria Domenica Cappellini, Professor of Internal Medicine, University of Milan
In this video, Professor Cappellini discusses the burden of chronic anaemia in patients with β-thalassaemia, including the varying impact of anaemia on transfusion-dependent and non-transfusion-dependent patients. Professor Cappellini also considers the impact of red blood cell transfusions on patients with β-thalassaemia including the effect on their psychological wellbeing.
8-minute video
Chronic anaemia in MDS
Doctor David Valcárcel, University Hospital Vall d’Hebron
In this video, Dr Valcárcel outlines the incidence, symptoms and treatments of chronic anaemia in patients with MDS. Dr Valcárcel also describes the role of ineffective erythropoiesis in the pathogenesis of chronic anaemia in MDS.
3-minute video
Complications of ineffective erythropoiesis in β-thalassaemia
Professor Olivier Hermine, Professor of Haematology, Paris Necker Children’s Hospital
In this video, Professor Hermine describes several complications associated with ineffective erythropoiesis in patients with β-thalassaemia. Professor Hermine also outlines the mechanisms of iron overload due to ineffective erythropoiesis and as a result of red blood cell transfusions, highlighting the resulting complications experienced by patients with β-thalassaemia.
5-minute video
Other haematological diseases
Aplastic anaemia
Aplastic anaemia is a blood disorder characterised by bone marrow failure causing an inability to produce blood cells and a deficit in haematopoietic stem cells and progenitor cells.11,12 This leads to pancytopenia and various symptoms such as fatal anaemia, bleeding and infection.11,12 The causes of aplastic anaemia include viral infection, environmental toxins and genetic mutations in genes affecting cellular mechanisms, which lead to bone marrow failure through physical or chemical damage, immune destruction or constitutional genetic defects.11
Myelofibrosis
Myelofibrosis is a myeloproliferative neoplasm characterised by ineffective stem cell-derived clonal haematopoiesis, bone marrow stromal reaction including reticulin fibrosis, abnormal cytokine expression, and extramedullary haematopoiesis.13 This leads to a vast array of symptoms including hepatosplenomegaly and severe anaemia.13 Ineffective erythropoiesis is the main cause of anaemia and it is thought that the aberrant cytokine production and host immune reaction contribute to this.13
Sickle cell anaemia
Sickle cell disease describes a group of inherited disorders characterised by abnormal haemoglobin molecules, haemoglobin S, which are caused by a point mutation in the β-globin chain.14 In sickle cell anaemia, the most common form of sickle cell disease, both β-globin subunits of the haemoglobin molecule are replaced by haemoglobin S.15 This leads to intravascular vaso-occlusion, stroke, priapism, and acute chest syndrome.14 Symptoms vary from person to person with some experiencing mild symptoms and others encountering more serious complications.15
Congenital dyserythropoietic anaemias
Congenital dyserythropoietic anaemias belong to a group of inherited conditions characterised by anaemia due to ineffective erythropoiesis with distinct morphological abnormalities of erythroblasts.16 These disorders result in variable degrees of anaemia without additional cytopenias.17
Inherited sideroblastic anaemias
Sideroblastic anaemia includes a group of heterogeneous disorders, characterised by the accumulation of iron in immature erythroid cells, which are referred to as ringed sideroblasts.3 The ineffective erythropoiesis characteristic of patients with inherited sideroblastic anaemia is caused by mutations in the genes involved in the initial stages of haem synthesis. Reduced haemoglobin and iron overload cause disease symptoms that range from mild to severe.3,18